A survivalist guide to paediatric central venous access device dysfunction
By Amanda Ullman, Tricia Kleidon, Anna Dean and the Paediatric Vascular Assessment and Management Service, Lady Cilento Children's Hospital, Brisbane.
This blog post was originally published in Don't Forget the Bubbles! http://dontforgetthebubbles.com/cvads-a-survival-guide/
We all love reliability. Central venous access devices (CVADs) are everywhere - across disciplines and departments, and we just want them to work reliably, without complication.
But every day, somewhere in your hospital, we are problem solving CVADs gone awry. And in many hospitals, no specialist vascular access teams are there to help you.
Being a CVAD survivalist will help you, most likely at 3am. Some situations will need escalating to specialists, but many can be quickly and effectively managed with simple, evidence-based techniques.
1. Needling a totally implanted device (ports)
Some totally implanted devices or ports are a pain. This is especially a problem in children with large amounts of adipose tissue, or poorly positioned ports.
But when problem solving this, everyone is different. Ask the child to sit up in the bed (or on their parent), and take off any restrictive clothing (e.g., bras for teenage girls). Use a rolled up towel under their back/shoulder blade and ask the patient to push their chest out, allowing less tissue to cover the port, making the port become more prominent. Make sure you have a firm grip of the port and stretch the skin out over it to reduce the amount of tissue you have to go through; this tip cannot be overemphasised. There should be no slack in the skin. You may need to change your grip a couple of times to get this just right. Also consider your own position when inserting; often placing yourself at the head of the bed is helpful.
2. Post CVAD insertion bleeding
Bleeding after the insertion of CVADs can cause frequent dressing changes, which is not the easiest task on a post-anaesthetic child or toddler.
The application of small drops of medical-grade superglue, or tissue adhesive (cyanoacrylate), directly on the CVAD insertion site results in immediate haemostasis, without resulting in significant skin injury [1, 2]. Most practical on peripherally inserted central catheters (PICCs) and non-tunnelled CVADs, make sure the site is completely dry before applying the glue, try not to stick yourself to the child or the CVAD, and allow the glue to dry completely before covering it with the usual CVAD dressing.
3. Lumens that won't aspirate or flush
Many factors can result in blocked CVAD lumens. A step-by-step approach is necessary[3].
a. Don't over complicate matters! Check for external occlusion due to a kinked line etc.
b. Change the needleless access device (i.e., the bung); these frequently dysfunction and result in blockage.
c. Try small, pulsatile aspirates, and then flushes of normal saline using a 10 mL syringe. Never use a syringe smaller than 10 mL or be tempted to use excessive force; this can result in catheter breakage. Ask the patient to cough, breathe deeply, or change their position while aspirating and flushing.
d. Assess for correct placement (chest x-ray, angiography).
e. Instil a thrombolytic agent, such as Urokinase or Alteplase (unless contraindicated), allow it to dwell for at least 60 minutes, and then aspirate and/or flush with normal saline. This may need to be repeated several times.
f. In the case of total occlusion where you can't administer a thrombolytic agent by a simple push, use a 3-way tap and additional empty 10 mL syringe. Turn the 3-way tap off to the thrombolytic agent, pull back on the empty 10 mL syringe to create a vacuum. Turn the tap so it is open to the drug and patient, and the drug should infuse under negative pressure.
g. If the blockage is a result of drug precipitation or build of lipid products; talk to the pharmacist for an appropriate dissolving agent such as hydrochloric acid or sodium bicarbonate.
h. Phone a friend, preferably someone who can insert a replacement device.
4. Local CVAD site irritation vs local infection
Identification is of the issue is key.
If there are any signs of inflammation or infection (e.g., raised red area, ooze: see Figure 1) take a swab for microscopy, culture and sensitivity (MCS). For uncomplicated exit site infections (i.e., no signs of systemic infection, purulent drainage or positive blood cultures) in long-term CVADs, the Infectious Diseases Society of America recommends the use of topical antimicrobial agents specific to the MCS results [4], (i.e., mupirocin ointment for S. aureus infection and ketoconazole or lotrimin ointment for Candida infection). If it is a short-term CVAD (e.g., PICC) take it out and organise a replacement device.
Figure 1: Early exit site infection

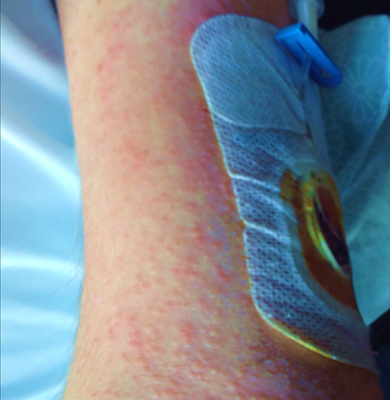
If infection doesn't seem likely, identify what is causing the skin irritation (see Figure 2). Most frequently it will be the decontaminant (2% CHG in alcohol) that has not been left to dry adequately. Some patients have a reaction to the fibres in the decontaminant stick. If this is a possibility use bottled (2% CHG in alcohol) with gauze and forceps. Additionally, consider the use of a barrier film product, provide symptom relief (i.e., itch, pain), and if symptoms persist recommend changing to a less-irritating silicone-based dressing product.
Figure 2: Contact dermatitis
5. Broken lumens
Oh God, it snapped. This happens a lot it seems.
Broken lumens don't always result in the end of the entire CVAD, but it does depend on the type of CVAD. Silicone CVADs, such as HickmansTM, have catheter repair kits that sit with skilled clinicians, such as paediatric oncology and haematology. Peripherally inserted central catheters vary by brand and catheter material in their ability to be repaired. This is definitely a phone a friend situation. When repairing a broken catheter, always consider the circumstances in which it fractured and environmental exposure. Blood cultures and prophylactic antibiotics might reduce the risk of subsequent infection.
References
1. Rickard, C.M., et al., A 4-arm randomized controlled pilot trial of innovative solutions for jugular central venous access device securement in 221 cardiac surgical patients. Journal of Critical Care, 2016. 36: p. 35-42.
2. Ullman, A.J., et al., Central venous Access device SeCurement And Dressing Effectiveness (CASCADE) in paediatrics: protocol for pilot randomised controlled trials. BMJ Open, 2016. 6(6).
3. Simcock, L., Managing occlusion in central venous catheters. Nurs Times, 2001. 97(21): p. 36-8.
4. Mermel, et al., Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis, 2009. 49: p. 1-45.
| Tags:IV managementvascular access devices |