Peripheral IntraVenous Catheter (PIVC)
What it is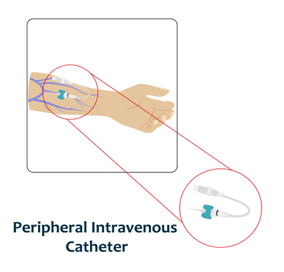
-
A short plastic tube inserted into a hand or arm, or the foot in babies and small children. Ultrasound guided insertion is recommended when no visible or palpable veins are present, for small children and people with fragile or compromised veins. Also called a "cannula", "drip" or "IV".
What it is used for
-
Short-term (< 7 days) delivery of intravenous fluids and medications. Not all medication can be infused through these catheters and if you are unsure you should check with your doctor or nurse.
Potential complications
-
Pain, tenderness, inflammation of the vein, blockage, blood clot, dislodgement, possible infection, fluid leaking from the vein into the tissues
How to prevent complications
- Wash hands before touching the device.
- Apply local anaesthetic cream 15-30 minutes before insertion.
- Avoid insertion in areas that bend (wrist, elbow).
- Clean the skin with an antiseptic solution before the device is inserted.
- The nurse/doctor accessing the PIVC should avoid touching the end of the line to limit risk of infection once its been cleaned.
- Ensure the dressing remains clean, dry and intact
- Assess the site every time it is accessed, at each shift or hourly if fluids are running for complications.
- Remove if complications occur and as soon as it is no longer needed.
- Remove immediately if possible infection (e.g. new temperature or pus from insertion site)
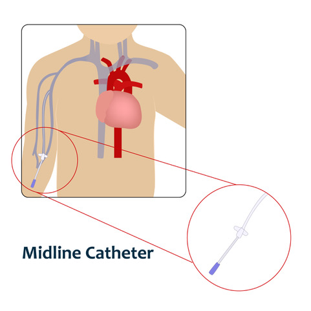
Midline
What it is
-
A plastic tube of medium length inserted into a vein in the upper arm (above the elbow) and stopping at the largest vein in the upper arm before the shoulder joint.
What it is used for
-
Medium term (5-7 days; can remain for several weeks) delivery of intravenous fluids, medications, some modified nutrition, and blood sampling.
Potential complications
-
Pain, tenderness, inflammation of the vein, blockage, blood clot, partial or complete dislodgement, or infection.
How to prevent complications
- Wash hands before touching the device.
- Use a securement device to anchor (secure) the catheter, in addition to the dressing to protect from infection.
- Replace the dressing when it is not clean, dry and intact, and routinely at 7days.
- Clean the needleless connector (end) with an antiseptic wipe and allow it to fully dry before connecting any syringes or lines.
- The nurse/doctor accessing the midline should avoid touching the end of the line to limit risk of infection once its been cleaned.
- Flush the line with normal saline before and after each use, using a stop/start technique.
- Assess the device daily whether in use or not, and during each administration for complications.
- Consider removal of the device if complications occur or when the device is no longer needed
- Remove immediately if possible infection (e.g. new temperature or pus from insertion site)
Peripherally Inserted Central Catheter (PICC)
What it is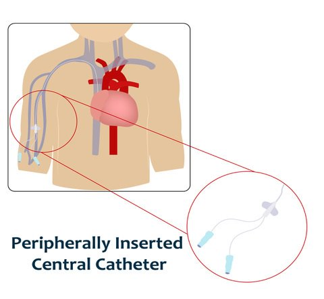
-
A plastic tube of medium length inserted into a vein in the upper arm (above the elbow) and stopping at the largest vein in the upper arm before the shoulder joint.
What it is used for
-
Medium term (5-7 days; can remain for several weeks) delivery of intravenous fluids, medications, some modified nutrition, and blood sampling.
Potential complications
-
Pain, tenderness, inflammation of the vein, blockage, blood clot, partial or complete dislodgement, or infection.
How to prevent complications
- Wash hands before touching the device.
- Use a securement device to anchor (secure) the catheter, in addition to the dressing to protect from infection.
- Replace the dressing when it is not clean, dry and intact, and routinely at 7 days.
- Clean the needleless connector (end) with an antiseptic wipe and allow it to fully dry before connecting any syringes or lines.
- The nurse/doctor accessing the midline should avoid touching the end of the line to limit risk of infection once its been cleaned.
- Flush the line with normal saline before and after each use, using a stop/start technique.
- Assess the device daily whether in use or not, and during each administration for complications.
- Consider removal of the device if complications occur or when the device is no longer needed.
-
Remove immediately if possible infection (e.g. new temperature or pus from insertion site)
Non-tunnelled Central Venous Catheter (nt-CVC)
What it is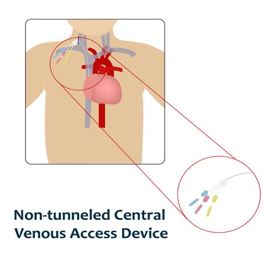
-
A hollow, plastic tube, inserted via a vein in the neck, chest, or groin into a large vein. Also called a "Central line" or "Central venous access device".
What it is used for
-
Short-medium term delivery of intravenous fluids, medications, nutrition or chemotherapy, and blood sampling.
Potential complications
-
Pain, lung puncture, blockage, blood clot, partial or complete dislodgement, internal movement of the tip into the wrong location, bleeding, infection, air embolus.
How to prevent complications
- Wash hands before touching the device.
- Use a securement device and dressing to anchor (secure) the catheter and any tubing.
- May have an anti-microbial disc or dressing to prevent infection.
- Replace the dressing when it is not clean, dry and intact, and routinely at 7 days.
- Clean the needleless connector(end) with an antiseptic wipe and allow it to fully dry before connecting any syringes or lines.
- The nurse/doctor accessing the catheter should avoid touching the end of the line to limit risk of infection once its been cleaned.
- Flush the line with normal saline before and after each use, using a stop/start technique.
- Assess the device daily whether in use or not, and during each administration for complications.
- Consider removal of the device if complications occur or when the device is no longer needed.
-
Needs to be removed lying down to avoid danger of air embolus.
Tunnelled cuffed Central Venous Catheter (tc-CVC)
What it is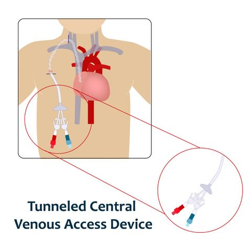
-
A long, hollow, plastic tube, inserted into a large central vein, usually in the neck or chest. A short tunnel is created on the anterior chest wall for the catheter to exit. This catheter has a cuff attached to it, that in time will adhere to the internal tissue to help prevent the catheter falling out. Also called a "Hickmans" or "Broviac" catheter.
What it is used for
-
Long term (> 3 months) delivery of intravenous fluids, medications, nutrition or chemotherapy, and sometimes blood sampling
Potential complications
-
Lung puncture, blockage, blood clot, partial or complete dislodgement, internal movement of the tip into the wrong location, bleeding, infection, air embolus.
How to prevent complications
- Wash hands before touching the device.
- Use a securement device and dressing to anchor (secure) the catheter for the first 3 months. After the cuff has adhered (around 3 months), sometimes can be left without a dressing.
- Replace the dressing when it is not clean, dry and intact, and routinely at 7days.
- Clean the needleless connector (end) with an antiseptic wipe and allow it to fully dry before connecting any syringes or lines.
- The nurse/doctor accessing the device should avoid touching the end of the line to limit risk of infection once its been cleaned.
- Flush the line with normal saline before and after each use, using a stop/start technique.
- Assess the device daily whether in use or not, and during each administration for complications.
-
Consider removal of the device if complications occur or when the device is no longer needed.
Tunnelled (non-cuffed) Central Venous Catheter (tnc-CVC)
What it is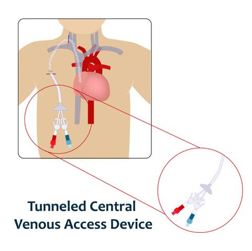
-
A long, hollow, plastic tube inserted into a large central vein, usually in the neck or chest. A short tunnel is created on the anterior chest wall for the catheter to exit.
What it is used for
- Short term dwell when peripheral veins are insufficient to provide necessary treatment.
- Medium to long term infusion of intravenous fluids, medications, nutrition or chemotherapy, and sometimes blood sampling.
-
Does not require a general anaesthetic to remove as does not have a cuff.
Potential complications
-
Lung puncture, blockage, blood clot, partial or complete dislodgement, internal movement of the tip into the wrong location, bleeding, infection, air embolus.
How to prevent complications
- Wash hands before touching the device.
- Use a securement device and dressing to anchor (secure) the catheter and lines.
-
Replace the dressing when it is not clean, dry and intact, and routinely at 7days.
Clean the needleless connector (end) with an antiseptic wipe and allow it to fully dry before connecting any syringes or lines. - The nurse/doctor accessing the device should avoid touching the end of the line to limit risk of infection once its been cleaned.
- Flush the line with normal saline before and after each use, using a stop/start technique.
- Assess the device daily whether in use or not, and during each administration for complications.
- Consider removal of the device if complications occur or when the device is no longer needed.
Totally implanted venous port device
What it is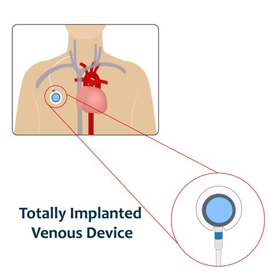
-
A small medical device surgically implanted under the skin of the chest and connected by a catheter to a deep central vein in the chest. Also called a "Port-a-cath".
What it is used for
-
Long term (months to years) delivery of intravenous fluids, medications, blood products, nutrition or chemotherapy, and sometimes blood sampling
Complications
-
Lung puncture, blockage, blood clots, partial or complete dislodgement, internal malposition, bleeding, infection, air embolus.
How to prevent complications
- Wash hands before touching the device.
- Apply local anaesthetic to the skin before insertion of the special PORT needle.
- Clean the skin with antiseptic solution and ensure it is dry before the needle is inserted into the port.
- Use a dressing to anchor the PORT needle and protect from infection.
- Replace the dressing if it is not clean, dry and intact, and routinely at 7days.
- Replace the port needle every 7 days or if a blockage in the port needle is suspected.
- The nurse/doctor accessing the device should avoid touching the end of the line to limit risk of infection once its been cleaned.
- Assess the device daily whether in use or not, and during each administration for complications.
-
The line should be flushed with normal saline after each use and the port locked with heparin after therapy is completed and every 4-6 weeks (depending on hospital policy).
Haemodialysis tunnelled cuffed Central Venous Catheter (Htc-CVC)
What it is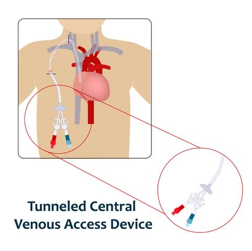
-
A long, hollow, plastic tube, inserted into a large central vein, usually in the neck or chest. A short tunnel is created on the anterior chest wall for the catheter to exit. This catheter has a cuff attached to it, that in time will adhere to the internal tissue to help prevent the catheter falling out.
What it is used for
-
Long term haemodialysis. To do this, the catheter has two separate openings inside; one to draw blood from the vein and out of the body into the dialysis pathway and the other allows cleaned blood to return to the body.
Potential complications
-
Lung puncture, blockage, blood clot, partial or complete dislodgement, internal movement of the tip into the wrong location, bleeding, infection, air embolus.
How to prevent complications
- Wash hands before touching the device.
- Use a securement device to anchor (secure) the catheter, in addition to the dressing to protect from infection.
- Replace the dressing when it is not clean, dry and intact, and routinely at 7days.
- Only specially trained dialysis nurses or doctors should access the device, unless in an emergency situation.
- Clean the needleless connector (end) with an antiseptic wipe and allow it to fully dry before connecting any syringes or lines.
- The nurse/doctor accessing the device should avoid touching the end of the line to limit risk of infection once its been cleaned.
- Flush the line with normal saline before and after each use, using a stop/start technique.
- Lock the catheter with an appropriate solution (e.g. heparin) at the completion of each session
- Assess the device daily whether in use or not, and during each administration for complications.
- Consider removal of the device if complications occur or when the device is no longer needed.